Allegro
‘Medicare for All’ — a vexing slogan
VIEWS FROM THE BOARD
Volume 124, No. 4April, 2024
Last summer the AFM Convention passed a resolution to endorse “Medicare for All,” in spite of the fact that it was poorly defined. I served on the committee that was assigned to vet this proposal.
Let me open by saying the U.S. healthcare system is a mess. Among other problems, it is based on steady employment, so it does not work for freelancers like performing artists. Moreover, people lose their coverage at the time they are most financially vulnerable — when they lose their jobs.
We need to fix this. The question is how?
I decided to stay silent on the resolution, which was passed by a voice vote at the convention. Several delegates from red states approached me afterwards to say this idea would never fly in their states.
Later, in the February 2024 issue of the International Musician, the lead proponent of this resolution took a swipe at my committee by saying we tried to “water down” the proposal, so I am choosing to speak up now.
BACKGROUND
The most recent “Medicare for All” proposal is HR 3421. It reads like a wish list:
- Automatic enrollment
- No out of pocket cost
- An ombudsman
- No private insurance
- Caps on pricing
There are causes for concern. The bill tries to address reproductive rights and gender care but it conflicts with a number of state laws as well as the federal Hyde Amendment (no relation) which forbids taxpayer dollars from funding abortions. There may be other challenges from state governments, which have more sovereignty than do provinces in most countries. Assuming the bill could ever overcome a Senate filibuster and become law — and putting aside for now the financing and cost (which is not defined in this bill) — it seems unlikely to pass a challenge in the Supreme Court.
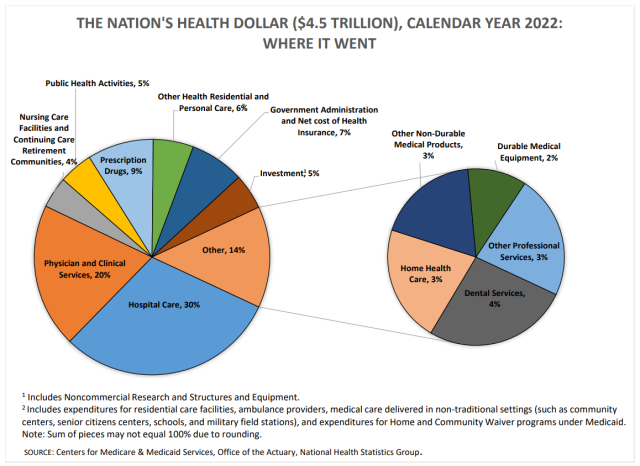
The U.S. spends $4.5 trillion a year on health care and only 7 percent is insurance overhead.
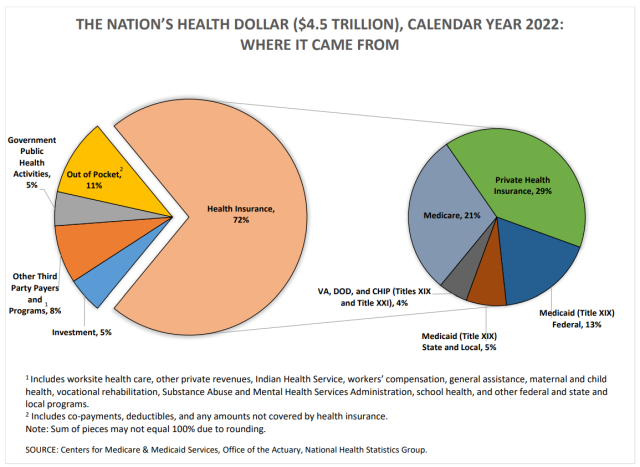
This chart shows the annual $4.5 trillion health care expenditure in the U.S., which is up $1 trillion since 2014. Click here to view both charts as a high-resolution PDF.
THE CLAIMS
Here are some reasons that proponents claim we need “Medicare for All”:
- The U.S. spends far more on health care than other rich countries but the outcomes are worse. This is true, but the costs are not driven by health insurance. Instead, the costs are driven by the actual cost of the healthcare services themselves. The U.S spends $4.5 trillion a year on health care and only 7 percent is insurance overhead. The poor outcomes are related to uneven coverage and because the U.S. “has the highest rate of people with multiple chronic conditions and an obesity rate nearly twice the OECD average.”
- All other rich countries use a “single-payer” system. This is a myth. Switzerland uses a non-centralized system of nonprofit health insurers. The German system is composed of non-governmental “sickness funds,” and is also decentralized. The Netherlands merges private and public insurance. All three countries have universal or close to universal coverage, and all three control rising costs. This proposed bill actually goes much further than most countries do. “Medicare for All proposals would leapfrog over other countries in terms of essentially eliminating private insurance and out-of-pocket costs, and providing very expansive benefits,” said Larry Levitt, a health policy expert with the nonpartisan Kaiser Family Foundation. “It raises questions about how realistic the proposals are.”
- The Affordable Care Act (ACA) doesn’t go far enough. This is true, largely because of states that haven’t expanded Medicaid and because the U.S. has failed to control healthcare inflation. (See this chart showing the U.S. annual $4.5 trillion expenditure, up $1 trillion since 2014.) However, enrollment in the ACA was up 33 percent this year over last year. The percentage of uninsured Americans has fallen from 46.5 million when the ACA was passed to 26 million and 10 states have brought the uninsured percentage down to 5 percent.
- This is the “only movement” for health care reform. This baffling argument was made at the convention. We are in a presidential election year and the dominant issues seem to be immigration, inflation (driven by food prices and real estate), reproductive rights, and the wars in Gaza and Ukraine. When it comes to health care, according to Gallup, “the majority of Americans recognize that the government has a role in expanding health insurance coverage, but many are ambivalent about fulfilling that role with a government-run system.”
- The AFL-CIO has endorsed “Medicare for All,” so the AFM should follow suit. Well…not exactly. This is how AFL-CIO Resolution #10, which passed in the June 2022 convention, reads: “Our goal is to move toward a single-payer system, like Medicare for All, that provides universal coverage using a social insurance model while retaining the critical role of workers’ health plans…not diminish the hard-fought benefits union members have won for themselves and all working people…provide multiemployer and other worker health plans the opportunity to administer core health benefits and to provide supplemental benefits, each on a fully tax advantaged basis…We will support legislation, like Medicare for All, that guarantees health care as a human right through a single-payer system, which we will judge according to the above core values” (emphasis added). This directly conflicts with the language in the proposed law: “private health insurers and employers may only offer coverage that is supplemental to, and not duplicative of, benefits provided under the program” (emphasis added). These two priorities cannot co-exist. Hence my opinion that this whole idea is poorly defined.
POSSIBLE SOLUTION: AN “ALL-PAYER SYSTEM”
So what are some possible solutions? One that might be easier to implement in the U.S. is an “all-payer” system. Researchers say that “an all-payer system would keep in place our many public and private insurers, but would require that they each pay the same price to providers.” The state of Maryland has already done this and has had success bringing down costs, which are the main barrier for most people.
This strategy sidesteps a federal government takeover, which, according to Gallup, makes most Americans uncomfortable. But an all-payer system evens the playing field for providers, payers and patients while also bringing down costs.
This is what my committee had in mind last summer when we proposed passing a resolution that called for a universal healthcare system in the U.S., not a “watered down” proposal as the proponent of the original resolution claims. There are a number of successful models in other countries, one or more of which might be a good fit for the U.S. political system and culture. We should study them and see which model that might be. Our committee’s proposal allows for using political capital to look for a solution that could work here, rather than chasing unicorns.
Local 802 Executive Board member Martha Hyde was a delegate to the 2023 AFM Convention. Among other duties, she serves as a trustee on the Local 802 Musicians Health Fund.
Opinion pieces in Allegro, including VIEWS FROM THE BOARD, do not necessarily reflect the views of other board members, officers, members or staff of Local 802. To inquire about submitting a piece to Allegro, send an e-mail to Allegro@Local802afm.org